Neurofacile 1 : La Voie Pyramidale.
Summary
TLDRThis video explains the voluntary motor pathways in the human nervous system, focusing on the two-neuron structure of motor transmission. It details the function of the first motor neuron (N1), which connects the brain to the spinal cord, forming the pyramidal tract. The video also covers the topographic organization of motor functions in the brain, the effects of cortical lesions, and clinical implications for motor recovery. Additionally, it touches on the phenomenon of motor plasticity and the role of the corticospinal tract in controlling muscle movements. Future videos will delve into related topics like spasticity and motor rehabilitation.
Takeaways
- 🧠 Human voluntary motor control is transmitted through a fast neural pathway involving two neurons: N1 (central pathway) and N2 (peripheral pathway).
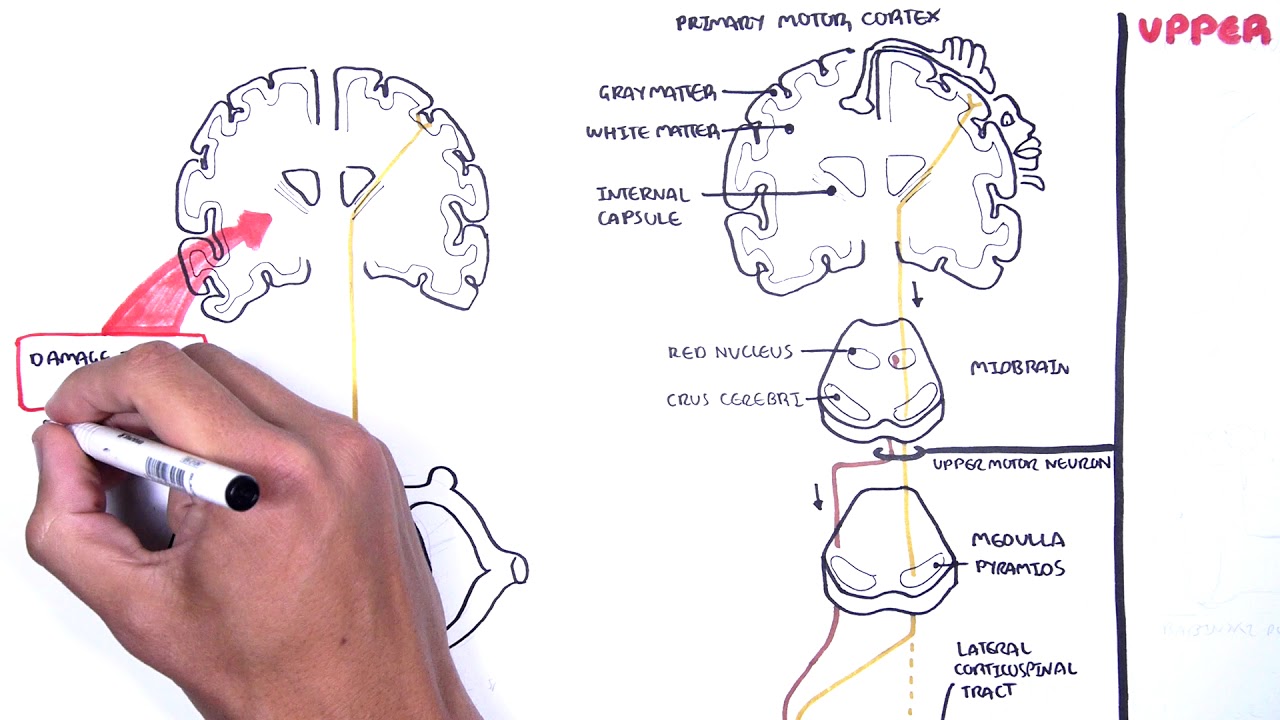
- 🦴 N1, or upper motor neurons, transmit signals from the brain to the spinal cord, forming part of the pyramidal tract, while N2 transmits from the spinal cord to muscles.
- 🔺 The pyramidal tract gets its name from the triangular shape of the cell bodies located in the motor cortex.
- 🌍 N1 axons descend through the white matter, crossing at the base of the medulla, and synapse in the anterior horn of the spinal cord with N2.
- 🖐️ The motor cortex is organized topographically, with each area corresponding to specific body parts, forming the motor homunculus.
- 💡 Topographical organization helps understand vascular hemiplegias, with specific arteries (middle cerebral and anterior cerebral) supplying different regions of the motor cortex.
- 🩸 A stroke in the middle cerebral artery affects the upper body and face, while one in the anterior cerebral artery affects the lower body.
- ♻️ Cortical plasticity allows adjacent areas to compensate for motor function loss after damage, aiding in post-injury motor recovery.
- 🔀 90% of pyramidal tract fibers cross at the medulla (decussation), controlling the contralateral side of the body, while 10% remain uncrossed, innervating the ipsilateral side.
- 🤸 The direct corticospinal tract ensures rapid recovery of axial muscle control due to double innervation from both hemispheres.
Q & A
What are the two types of motoneurons involved in voluntary motor activity?
-The two types of motoneurons involved are upper motoneurons (N1), which transmit signals from the brain to the spinal cord, and lower motoneurons (N2), which transmit signals from the spinal cord to the muscles.
Where are the cell bodies of upper motoneurons located?
-The cell bodies of upper motoneurons (N1) are located in the grey matter of the brain, specifically in the motor cortex.
What is the pyramidal tract and how is it named?
-The pyramidal tract is a collection of axons that transmit motor signals from the motor cortex to the spinal cord. It is named after the triangular shape of the cell bodies that form it.
What is the role of the internal capsule in the transmission of motor signals?
-The internal capsule is a region in the brain where the axons of the upper motoneurons (N1) gather and concentrate before descending to the spinal cord. It plays a crucial role in transmitting motor signals to the body.
How does the somatotopic organization of the motor cortex influence motor control?
-The motor cortex is organized somatotopically, meaning that specific areas of the cortex control specific parts of the body. This organization creates a topographic map, where larger areas control more finely controlled parts like the hands and face.
What happens when there is an interruption of blood flow to the middle cerebral artery?
-An interruption of blood flow to the middle cerebral artery can cause hemiplegia, particularly affecting the upper limbs and face, as this artery supplies the lateral part of the motor cortex responsible for these areas.
What is the difference between proportional and non-proportional hemiplegia?
-Proportional hemiplegia affects the entire half of the body equally and typically results from lesions in the subcortical regions, whereas non-proportional hemiplegia varies in intensity across different body parts and indicates a cortical lesion.
How does brain plasticity aid in motor recovery after a lesion?
-Brain plasticity allows adjacent areas of the cortex to take over the function of damaged regions, such as when a hand's motor function is partially restored by nearby areas following a lesion.
What is the decussation of the pyramids, and why is it important?
-The decussation of the pyramids refers to the crossing of the motor fibers at the base of the brainstem, which ensures that each cerebral hemisphere controls the opposite side of the body. It is crucial for understanding the location and effects of motor impairments.
How does the corticospinal tract ensure balance control after hemisphere lesions?
-Balance control is maintained after lesions in one hemisphere because the axial muscles receive dual innervation from both the crossed and uncrossed corticospinal fibers, allowing rapid recovery of postural control.
Outlines

هذا القسم متوفر فقط للمشتركين. يرجى الترقية للوصول إلى هذه الميزة.
قم بالترقية الآنMindmap

هذا القسم متوفر فقط للمشتركين. يرجى الترقية للوصول إلى هذه الميزة.
قم بالترقية الآنKeywords

هذا القسم متوفر فقط للمشتركين. يرجى الترقية للوصول إلى هذه الميزة.
قم بالترقية الآنHighlights

هذا القسم متوفر فقط للمشتركين. يرجى الترقية للوصول إلى هذه الميزة.
قم بالترقية الآنTranscripts

هذا القسم متوفر فقط للمشتركين. يرجى الترقية للوصول إلى هذه الميزة.
قم بالترقية الآنتصفح المزيد من مقاطع الفيديو ذات الصلة

NEUROFISIOLOGIA - AS GRANDES VIAS AFERENTES E EFERENTES - Prof Mara Ribeiro - Aula 13

Motor Pathways | Motor Neurons and Disease
Introduction to Upper and Lower Motor Neuron Lesions

Sistema nervoso (seconda parte).

Neuron materi lengkap - struktur, bentuk, fungsi, jenis - biologi sma kelas bab.sistem saraf

Anatomi Sistem Saraf: Saraf Pusat & Tepi | Neurologi
5.0 / 5 (0 votes)
