How to interpret an ECG systematically | EXPLAINED CLEARLY!
Summary
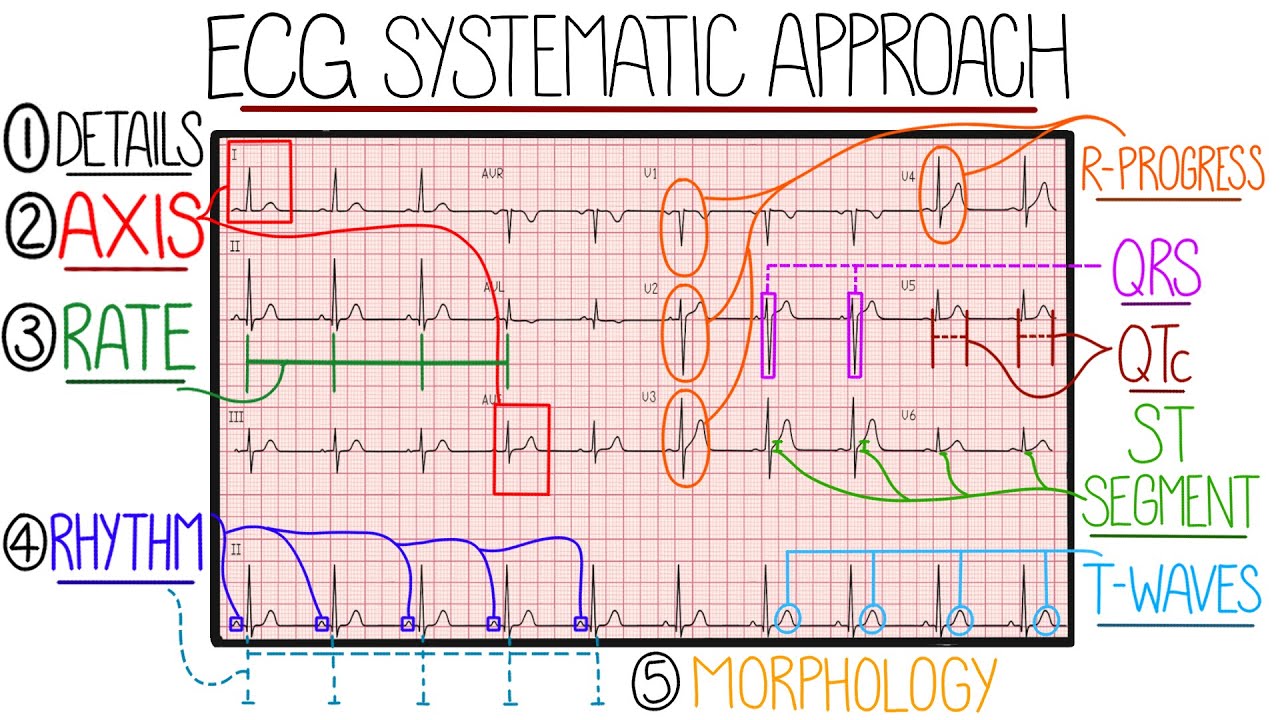
TLDRThis video tutorial offers a structured approach to interpreting ECGs, essential for medical students and junior doctors. It covers patient details, calibration checks, and a systematic method starting with rate, rhythm, and axis, followed by in-depth analysis of each ECG component. The guide also discusses common abnormalities, such as different types of heart blocks and myocardial infarction, providing a foundation for diagnosing cardiac conditions.
Takeaways
- 🔍 Always verify patient details and ECG calibration before interpretation to avoid errors and ensure accuracy.
- 📈 Calculate the heart rate using either the number of large squares in the RR interval or by counting QRS complexes over a 10-second rhythm strip.
- 💓 Understand the difference between regular and irregular rhythms, and identify specific conditions like second-degree AV block type 1 (Wenckebach phenomenon) and atrial fibrillation.
- 📊 Assess the cardiac axis using leads I, II, and III to determine if there's any left or right axis deviation, which can indicate certain cardiac conditions.
- 👀 Check the presence and appearance of P waves in all 12 leads to identify atrial activity and conditions like atrial fibrillation or atrial enlargement.
- ⏱️ Evaluate the PR interval to determine if there's first-degree heart block or other conduction delays.
- 🔊 Examine the QRS complex for width, height, and morphology to detect abnormalities like bundle branch blocks or myocardial infarctions.
- 📉 Look for ST segment deviations that could signify myocardial ischemia or infarction, distinguishing between STEMI and NSTEMI.
- 🌊 Assess T wave appearance to identify conditions like hyperkalemia, ischemia, or pulmonary embolism.
- ⏲️ Measure the QT interval and consider factors like heart rate and medication effects to identify potential risks for arrhythmias like Torsades de Pointes.
Q & A
What is the first step in interpreting an ECG according to the video?
-The first step is checking patient details using three pieces of identification, which is crucial as missing this step in exams could result in zero marks.
What should be the paper speed and amplitude calibration for a standard ECG?
-The paper speed should be 25 millimeters per second, with one small square equivalent to 0.04 seconds and one large square to 0.2 seconds. The amplitude calibration should be 10 millimeters per millivolt.
How can one calculate the heart rate on an ECG with a regular rhythm?
-For a regular rhythm, you can use the equation 300 divided by the number of large squares in the RR interval to calculate the heart rate.
What is the alternative method to calculate the heart rate if the rhythm is irregular?
-If the rhythm is irregular, you count the number of QRS complexes along the rhythm strip and multiply it by six, as the total length of the rhythm strip is 10 seconds.
What does a normal adult heart rate range from?
-A normal adult heart rate ranges from 60 to 100 beats per minute, with bradycardia being slower than this and tachycardia being faster.
How can you determine if the ECG rhythm is regular or irregular?
-You can determine the rhythm by placing a piece of paper above the start of the rhythm strip and marking three or four R waves, then moving the paper along the strip to see if the lines match up with subsequent R waves.
What does the term 'Wenckebach phenomenon' refer to in the context of ECG interpretation?
-The term 'Wenckebach phenomenon' refers to second-degree AV block type 1, where there is a predictable pattern of QRS complexes followed by a pause, often seen as two QRS complexes followed by a pause and then the same again repeated.
What does the cardiac axis represent and what is the normal range for it?
-The cardiac axis represents the average direction of electrical depolarization through the ventricles. In healthy individuals, this average direction is between -30 and positive 90 degrees in the coronal plane.
How can you identify if there's left axis deviation or right axis deviation on an ECG?
-You can identify axis deviation by comparing the QRS complexes in leads 1, 2, and 3. For a normal axis, lead 2 should be more positive than at least one of the other leads. In right axis deviation, lead 3 is more positive than lead 2 and 1, and in left axis deviation, lead 1 is more positive than lead 3 and 2.
What does the absence of P waves with an irregularly irregular rhythm indicate on an ECG?
-The absence of P waves with an irregularly irregular rhythm indicates atrial fibrillation, which is a common finding in medical school exams and clinical practice.
What is the normal duration of the PR interval and what does a prolonged PR interval indicate?
-A normal PR interval is 0.12 to 0.20 seconds or 3 to 5 small squares. A prolonged PR interval indicates first-degree heart block, which is caused by the AV node conducting electricity slower than normal.
What does a Delta wave in the QRS complex signify?
-A Delta wave in the QRS complex signifies an abnormality and can be seen in conditions such as Wolf Parkinson White syndrome.
What is the significance of a pathological Q wave on an ECG?
-A pathological Q wave, which is longer and taller than normal, often represents an old myocardial infarction.
What does ST segment elevation or depression on an ECG indicate?
-ST segment elevation or depression can indicate myocardial ischemia. If present in two or more contiguous leads, it suggests ischemia is likely present. ST elevation specifically can indicate a STEMI (ST elevation myocardial infarction).
What does the assessment of T waves on an ECG represent?
-The assessment of T waves on an ECG represents ventricular repolarization. Abnormal T waves, such as being tall, normal, or inverted, can indicate conditions like hyperkalemia, myocardial infarction, or pulmonary embolus.
What is the normal QT interval and why is it important to calculate the corrected QT interval?
-A normal QT interval is less than 440 milliseconds in men or less than 460 milliseconds in women. The corrected QT interval is calculated to standardize the QT interval to 60 beats per minute, accounting for variations due to heart rate.
Why is it important to assess the ECG components in all 12 leads?
-Assessing the ECG components in all 12 leads is important to avoid missing any abnormalities, as different leads provide different views of the heart's electrical activity.
Outlines

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowMindmap

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowKeywords

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowHighlights

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowTranscripts

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowBrowse More Related Video





5.0 / 5 (0 votes)