Urinary Specimen Collection, Incontinence, and UTI's - Fundamentals of Nursing | @LevelUpRN
Summary
TLDRIn this video, Meris covers key topics related to urinary health, including normal urine characteristics, specimen collection, urinary incontinence, and urinary tract infections (UTIs). She explains expected urine output, specific gravity, and abnormal signs such as cloudy or malodorous urine. Meris also discusses how to collect clean catch and 24-hour urine samples, different types of incontinence, and key risk factors and symptoms of UTIs, particularly in older adults. Practical tips for UTI prevention and patient teaching are provided, making this video essential for nursing students.
Takeaways
- 💧 Normal urine output should range from 0.5 to 1.5 mL per kg per hour, aiming for about 1,500 mL per day.
- ⚠️ Notify the provider if urinary output is less than 30 mL per hour, indicating severe oliguria.
- 🔬 Specific gravity of urine ranges from 1.005 to 1.030, with lower values indicating dilute urine.
- 🌫️ Urine should be clear, and cloudy or malodorous urine is considered abnormal.
- 🧪 A midstream clean catch urine specimen is essential for accurate results and requires specific instructions for patients with different anatomy.
- ⏳ For 24-hour urine collections, the first void of the day should be discarded, and the sample should be kept refrigerated.
- 💪 Stress incontinence is associated with increased intra-abdominal pressure and is more common in patients with weakened pelvic floor muscles.
- 🚻 Urge incontinence involves the inability to reach the bathroom in time, and treatments include physical therapy and medications.
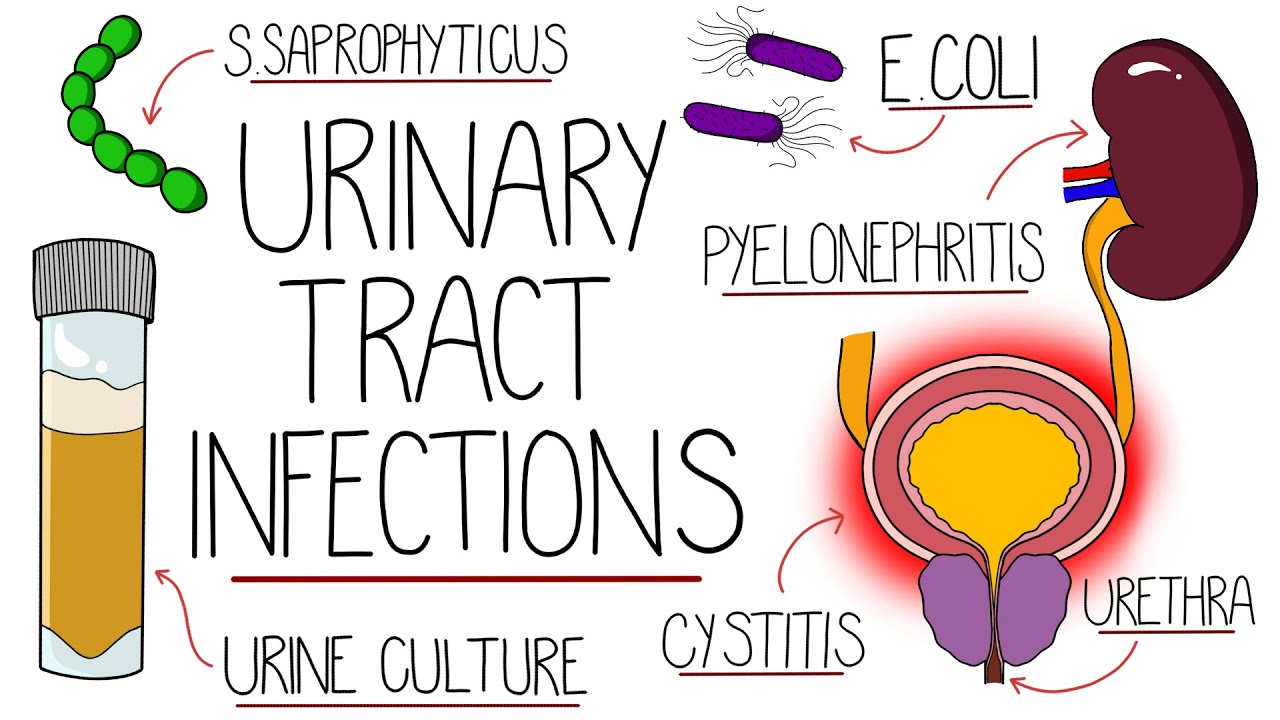
- ❗ People with a vulva are more at risk for urinary tract infections (UTIs) due to a shorter urethra.
- 🧼 Key UTI prevention tips include wiping front to back, wearing cotton underwear, avoiding bubble baths, and increasing fluid intake.
Q & A
What is the normal urine output per hour for a patient?
-The normal urine output is 0.5 to 1.5 milliliters per kilogram per hour, with a general goal of 1,500 mL or 1.5 liters per day.
When should a provider be alerted about a patient's urine output?
-The provider should be alerted if the patient's urine output is less than 30 mL per hour, as this indicates severe oliguria.
What does a low specific gravity in urine indicate?
-A low specific gravity (below 1.005) indicates dilute urine, meaning it is less concentrated.
How can you remember the relationship between dilute urine and specific gravity?
-Dilute urine starts with 'L,' and it corresponds to a low specific gravity, which also starts with 'L.'
What are the steps for a clean catch urine specimen for a patient with a penis?
-The patient should retract the foreskin if uncircumcised, clean around the urethral meatus, urinate into the toilet, stop, then urinate into the cup, and stop again to finish urinating into the toilet.
What patient education is important for a 24-hour urine specimen collection?
-The patient should discard the first void of the day, start collecting urine after that, and keep the container refrigerated.
Who is most at risk for stress urinary incontinence?
-Patients who have had multiple pelvic surgeries or multiple pregnancies and deliveries are most at risk due to weakened pelvic floor muscles.
What is the difference between stress incontinence and urge incontinence?
-Stress incontinence is urine leakage due to increased intra-abdominal pressure, such as from coughing or sneezing, while urge incontinence is the inability to make it to the bathroom in time when feeling the urge to urinate.
Who is most at risk for urinary tract infections (UTIs)?
-People with a vulva are at higher risk for UTIs because they have a shorter urethra, making it easier for bacteria to enter the urinary tract.
What is important patient teaching for preventing urinary tract infections?
-Patients should wipe from front to back, wear cotton underwear, avoid bubble baths, empty the bladder regularly, void after intercourse, increase fluid intake, and consider cranberry juice to help with UTI symptoms.
Outlines

Esta sección está disponible solo para usuarios con suscripción. Por favor, mejora tu plan para acceder a esta parte.
Mejorar ahoraMindmap

Esta sección está disponible solo para usuarios con suscripción. Por favor, mejora tu plan para acceder a esta parte.
Mejorar ahoraKeywords

Esta sección está disponible solo para usuarios con suscripción. Por favor, mejora tu plan para acceder a esta parte.
Mejorar ahoraHighlights

Esta sección está disponible solo para usuarios con suscripción. Por favor, mejora tu plan para acceder a esta parte.
Mejorar ahoraTranscripts

Esta sección está disponible solo para usuarios con suscripción. Por favor, mejora tu plan para acceder a esta parte.
Mejorar ahoraVer Más Videos Relacionados





5.0 / 5 (0 votes)
