Morphine Pharmacology: Mechanism of Action, Therapeutic Uses & Adverse Effects
Summary
TLDRThis lecture provides a comprehensive overview of morphine, the prototypical opioid, detailing its pharmacology, mechanisms of action, therapeutic uses, and adverse effects. It explains how morphine binds to μ, δ, and κ opioid receptors in the CNS and periphery to produce analgesia, euphoria, sedation, and respiratory depression. Peripheral effects on the cardiovascular, respiratory, gastrointestinal, urinary, endocrine, and immune systems are discussed. The video also covers tolerance, physical and psychological dependence, and critical contraindications, including head injury, asthma, hepatic impairment, and biliary colic. Practical clinical applications, such as pain management, pulmonary edema, and anesthesia, are highlighted, offering a complete guide to morphine’s pharmacological profile.
Takeaways
- 💊 Morphine is the prototypical natural opioid derived from the opium plant, first isolated in 1803, and acts primarily as a μ-opioid receptor agonist.
- 🧬 Opioids are classified into natural, semi-synthetic, and synthetic, with natural and semi-synthetic opioids acting as full agonists and synthetic opioids including agonists, antagonists, and partial agonists.
- ⚡ Morphine can be administered orally, intravenously, intramuscularly, or subcutaneously, with oral bioavailability around 25% due to significant first-pass metabolism.
- 🧠 Morphine produces analgesia via spinal (posterior horn), supraspinal (brain), peripheral, and psychological pathways, affecting both sensory and emotional components of pain.
- 😊 Central effects of morphine include analgesia, euphoria, sedation, respiratory depression, cough suppression, miosis, nausea, vomiting, pruritus, and hyperthermia.
- ❤️ Peripheral effects involve cardiovascular (bradycardia, hypotension), respiratory (bronchoconstriction), gastrointestinal (constipation, delayed motility), urinary (retention), biliary (colic), uterine (prolonged labor), endocrine (hormonal changes), and immune suppression.
- 🏥 Therapeutic uses of morphine include severe pain management (cancer, MI, surgery), acute pulmonary edema, anesthesia adjunct, and treatment of colic with spasmolytics.
- ⚠️ Adverse effects include respiratory depression, constipation, urinary retention, biliary colic, prolonged labor, tolerance, and both physical and psychological dependence.
- ⏱️ Morphine tolerance develops rapidly, affecting analgesia, sedation, respiratory depression, and gastrointestinal effects, often requiring opioid rotation for effective pain management.
- 🚫 Contraindications include head injury or increased intracranial pressure, bronchial asthma, hypovolemia, biliary colic, hepatic impairment, penile prosthetic hyperplasia, undiagnosed acute abdominal pain, and use in infants or elderly due to respiratory risks.
- 💉 Morphine dependence manifests as withdrawal syndrome (physical dependence) within hours if stopped abruptly, and psychological dependence as addiction with behavioral and motivational impairment.
- ⚖️ Morphine’s clinical use requires careful monitoring due to the narrow therapeutic window and potential for severe respiratory depression, especially in non-tolerant patients.
Q & A
What is morphine and from what is it derived?
-Morphine is the prototypical opioid analgesic, derived from the opium plant. It was first isolated in 1803, and its name comes from Morpheus, the Greek God of Dreams.
How are opioids classified and where does morphine fit?
-Opioids are classified into natural (e.g., morphine, codeine), semi-synthetic (e.g., heroin, oxycodone), and synthetic (e.g., fentanyl, naloxone). Morphine is a natural opioid and acts as a full agonist primarily at MU receptors.
What are the pharmacokinetics of morphine regarding administration, absorption, metabolism, and excretion?
-Morphine can be administered orally, intravenously, intramuscularly, or subcutaneously. Oral bioavailability is about 25% due to first-pass liver metabolism. It distributes rapidly to the brain, lungs, liver, and kidneys, has a half-life of 4–5 hours, is metabolized in the liver, and excreted mainly through the kidneys (90%) and bile (10%).
Which opioid receptors does morphine act on and what is its primary mechanism of analgesia?
-Morphine acts on MU, Delta, and Kappa opioid receptors, with the highest affinity for MU receptors. Analgesia occurs through four mechanisms: spinal analgesia (inhibition of substance P in the spinal cord), supraspinal analgesia (activation of descending inhibitory pathways in the brain), reduction of norepinephrine release (reducing psychological pain), and activation of peripheral opioid receptors in painful tissue.
What are the central nervous system effects of morphine?
-Central effects include analgesia, euphoria, sedation, respiratory depression, cough suppression, miosis, nausea and vomiting, temperature changes, and itching. Some effects, like respiratory depression, can be life-threatening.
How does morphine affect the gastrointestinal system?
-Morphine reduces gastrointestinal motility by increasing tone and decreasing propulsive movements in the stomach, small intestine, and large intestine. This leads to delayed transit and constipation, which is a major side effect in long-term use.
What are the cardiovascular and respiratory effects of morphine?
-Cardiovascular effects include bradycardia (via vagal stimulation) and hypotension (from histamine release). Respiratory effects include respiratory depression and bronchoconstriction, making morphine contraindicated in patients with asthma or chronic respiratory diseases.
What types of dependence can develop with morphine use?
-Morphine can cause physical dependence, which manifests as withdrawal symptoms when the drug is stopped, and psychological dependence, or addiction, which is characterized by compulsive drug-seeking behavior and impaired motivation.
What are the major contraindications for morphine use?
-Major contraindications include head injury or increased intracranial pressure, bronchial asthma, hypovolemia, hypotension, bradycardia, biliary colic, penile prosthetic hyperplasia, hepatic impairment, undiagnosed acute abdominal pain, and use in infants or elderly due to increased risk of respiratory depression.
Why does morphine tolerance develop and what is opioid rotation?
-Tolerance occurs due to neural adaptation and receptor regulation, requiring higher doses for the same effect. Opioid rotation involves switching between different opioids to restore analgesic efficacy in patients with chronic pain and prevent tolerance-related issues.
How does morphine affect the endocrine and immune systems?
-Morphine increases ADH, prolactin, and somatotropin secretion while inhibiting luteinizing hormone, leading to decreased testosterone, libido, and energy. It also suppresses natural killer cell and lymphocyte activity, reducing immunity and potentially worsening infections or cancer progression.
What are the mechanisms behind morphine-induced respiratory depression and miosis?
-Respiratory depression occurs by inhibition of the brainstem respiratory centers, leading to slower breathing and CO₂ retention. Miosis (pupil constriction) occurs due to vagal stimulation and parasympathetic activation, and severe pinpoint pupils indicate toxic doses.
Outlines

Cette section est réservée aux utilisateurs payants. Améliorez votre compte pour accéder à cette section.
Améliorer maintenantMindmap

Cette section est réservée aux utilisateurs payants. Améliorez votre compte pour accéder à cette section.
Améliorer maintenantKeywords

Cette section est réservée aux utilisateurs payants. Améliorez votre compte pour accéder à cette section.
Améliorer maintenantHighlights

Cette section est réservée aux utilisateurs payants. Améliorez votre compte pour accéder à cette section.
Améliorer maintenantTranscripts

Cette section est réservée aux utilisateurs payants. Améliorez votre compte pour accéder à cette section.
Améliorer maintenantVoir Plus de Vidéos Connexes

Opioides parte 1 | Aula 36 | Farmacologia do SNC rápida e fácil | Flavonoide

Curso de Farmacologia: Aula 7 - Farmacologia adrenergica - Agonistas e antagonistas diretos
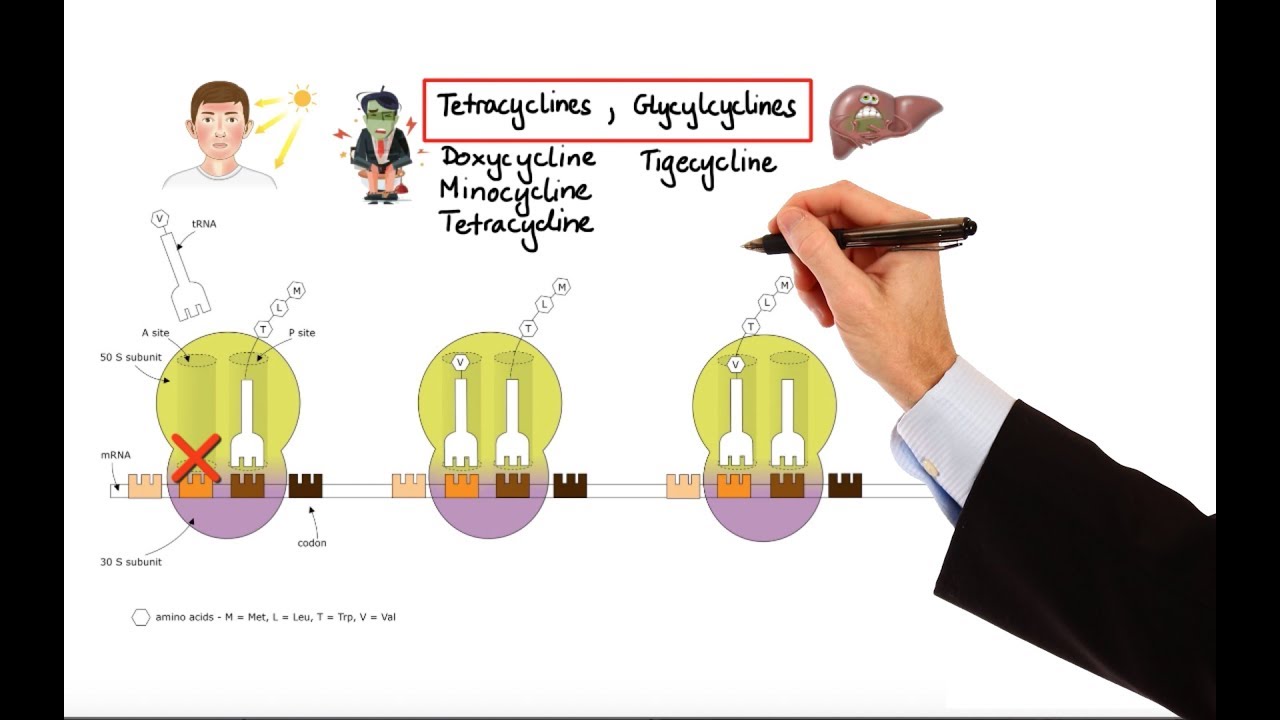
Pharmacology – ANTIBIOTICS – DNA, RNA, FOLIC ACID, PROTEIN SYNTHESIS INHIBITORS (MADE EASY)

Pharmacology - ANTIDEPRESSANTS - SSRIs, SNRIs, TCAs, MAOIs, Lithium ( MADE EASY)
Pharmaceutical Toxicology

TRAMADOL EXPLAINED - MECHANISM OF ACTION, USES, SIDE EFFECTS, DOSE
5.0 / 5 (0 votes)
