Pancreatite aguda na emergência: diagnóstico e conduta
Summary
TLDRThis video script provides a comprehensive guide to the diagnosis and emergency management of acute pancreatitis. It covers key clinical signs such as upper abdominal pain with radiation, nausea, and vomiting, and emphasizes the importance of early intervention. The script explains the pathophysiology, including enzyme activation and systemic inflammation, and outlines the primary causes: biliary issues and alcohol consumption. It details diagnostic criteria, including clinical presentation, lab tests, and imaging. The video also highlights initial treatment strategies, including fluid resuscitation, pain management, and nutritional support, while stressing the importance of monitoring for complications and organ dysfunction.
Takeaways
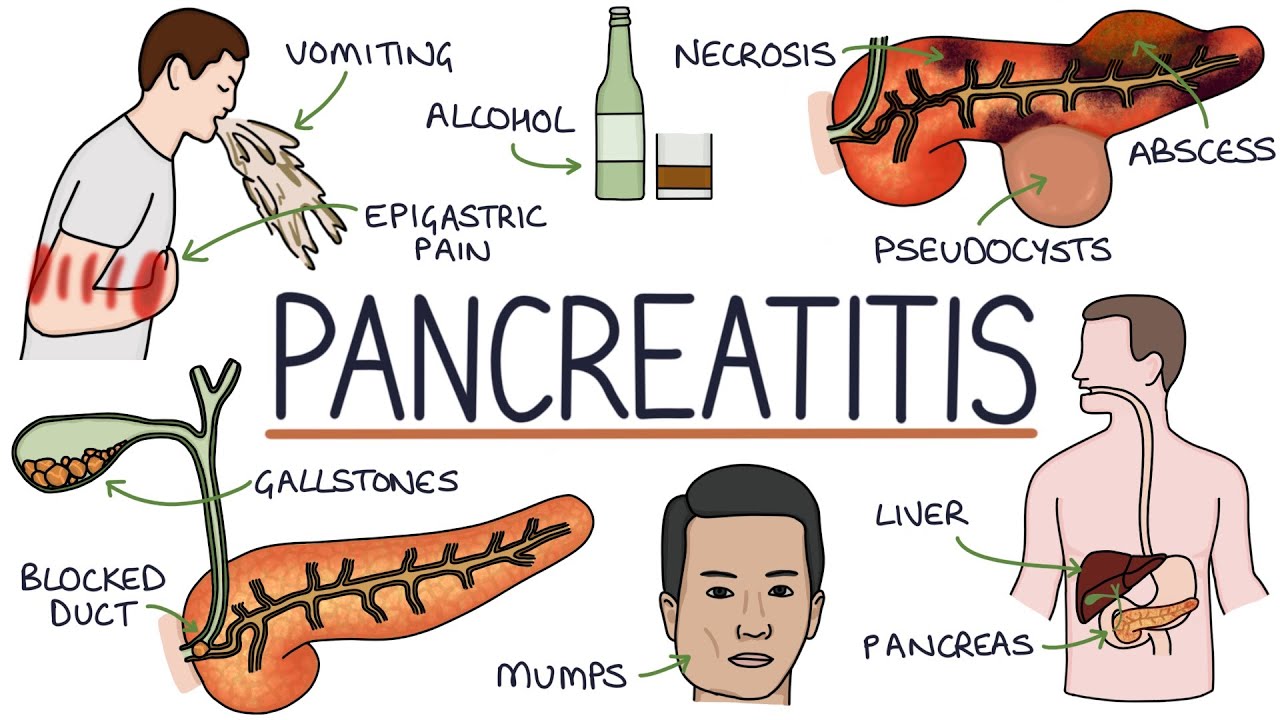
- 🧠 Acute pancreatitis is an inflammatory condition where pancreatic enzymes become activated prematurely, causing self-digestion of the pancreas.
- ⚠️ The most common causes are biliary obstruction (gallstones) and chronic alcohol use, with small migrating stones being particularly dangerous.
- 🔥 The disease can trigger a systemic inflammatory response (SIRS) due to enzymes entering the bloodstream, potentially leading to multi-organ dysfunction.
- 🧪 Diagnosis requires at least 2 of 3 criteria: typical abdominal pain, elevated amylase/lipase (>3x normal), or imaging findings.
- 📊 Severity is classified using the Atlanta criteria into mild, moderately severe, and severe based on the presence and duration of organ dysfunction.
- 🫁 Key indicators of organ dysfunction include oxygen saturation <94%, systolic blood pressure <90 mmHg, and elevated creatinine levels.
- 💧 Early and aggressive fluid resuscitation with Ringer lactate is the most critical initial treatment to prevent complications.
- 💊 Opioids like morphine are safe and effective for pain control, despite myths about sphincter of Oddi spasm.
- 🚫 Patients should initially be kept fasting, but early reintroduction of feeding (within 12–48 hours) is recommended depending on severity.
- 🍽️ Nutritional support should progress from oral feeding to enteral (nasoenteric tube) and finally parenteral if necessary.
- 🦠 Prophylactic antibiotics are not recommended in the early phase and should only be used if infected necrosis develops later.
- 🖥️ CT imaging is not always needed initially but is useful after 48–72 hours to assess complications and severity using the Balthazar score.
- 🏥 All patients should be hospitalized and closely monitored, ideally in a facility capable of managing complications.
- ⏱️ Complications like infected necrosis typically occur after 2–4 weeks, not in the initial phase of the disease.
- 🎯 Early recognition, severity assessment, and prompt supportive care significantly improve patient outcomes in acute pancreatitis.
Q & A
What clinical presentation should immediately raise suspicion for acute pancreatitis?
-Severe epigastric abdominal pain with a band-like distribution radiating to the back, often accompanied by nausea and vomiting, is highly suggestive of acute pancreatitis.
Why can pancreatitis lead to severe systemic complications?
-Because activated pancreatic enzymes leak into the bloodstream, causing widespread inflammation (SIRS), endothelial damage, and potentially multi-organ failure.
What are the two main functions of the pancreas relevant to pancreatitis?
-The pancreas has endocrine functions (hormone production) and exocrine functions (digestive enzyme secretion), both of which contribute to its importance and the severity of its inflammation.
What is the most common cause of acute pancreatitis?
-The most common cause is biliary obstruction due to gallstones, accounting for approximately 45–50% of cases.
How do gallstones trigger pancreatitis?
-Gallstones can obstruct or irritate the ampulla, leading to blockage of pancreatic enzyme outflow, increased ductal pressure, and premature activation of enzymes within the pancreas.
What criteria are used to diagnose acute pancreatitis?
-Diagnosis requires at least two of three criteria: typical abdominal pain, elevated amylase or lipase (≥3 times normal), and imaging findings consistent with pancreatitis.
How is the severity of pancreatitis classified according to the Atlanta criteria?
-It is classified as mild (no organ dysfunction), moderately severe (transient organ dysfunction <48 hours), or severe (persistent organ dysfunction >48 hours).
What simple clinical parameters help identify organ dysfunction in pancreatitis?
-Oxygen saturation below 94% (respiratory), systolic blood pressure below 90 mmHg (circulatory), and elevated creatinine (renal) indicate organ dysfunction.
What is the most important initial treatment for acute pancreatitis?
-Aggressive fluid resuscitation with Ringer lactate is the most important initial treatment to counteract hypovolemia and prevent organ failure.
How should pain be managed in patients with acute pancreatitis?
-Opioids such as morphine are recommended, and concerns about sphincter of Oddi spasm are not clinically significant.
Why is early aggressive hydration critical in pancreatitis?
-Because systemic inflammation increases capillary permeability, leading to fluid loss into tissues, requiring replacement to maintain adequate circulation and organ perfusion.
What is the recommended nutritional approach in pancreatitis?
-Start with fasting, then reintroduce a low-fat oral diet early if tolerated; if not, proceed to enteral feeding via tube, and lastly parenteral nutrition if necessary.
When should a CT scan be performed in pancreatitis?
-CT is not always needed initially but is useful after 48–72 hours in severe cases or when diagnosis is uncertain.
What is the Balthazar score used for?
-It is used to assess the severity of pancreatitis on CT imaging, considering inflammation and necrosis, with higher scores indicating worse prognosis.
Why are antibiotics not routinely used in early pancreatitis?
-Because early pancreatitis is typically sterile inflammation; antibiotics are reserved only for confirmed or suspected infected necrosis later in the disease course.
What are the major early and late complications of pancreatitis?
-Early complications include systemic inflammatory response and organ failure; late complications include infected necrosis, pseudocysts, and fluid collections.
Outlines

此内容仅限付费用户访问。 请升级后访问。
立即升级Mindmap

此内容仅限付费用户访问。 请升级后访问。
立即升级Keywords

此内容仅限付费用户访问。 请升级后访问。
立即升级Highlights

此内容仅限付费用户访问。 请升级后访问。
立即升级Transcripts

此内容仅限付费用户访问。 请升级后访问。
立即升级浏览更多相关视频
Understanding Pancreatitis

Acute Pancreatitis: pathogenesis, clinical findings, and complications

Acute exacerbation of asthma- management | Status asthmaticus|EMERGENCY MEDICINE|Pediatrics lecture

Pancreas Clinical Anatomy and Physiology
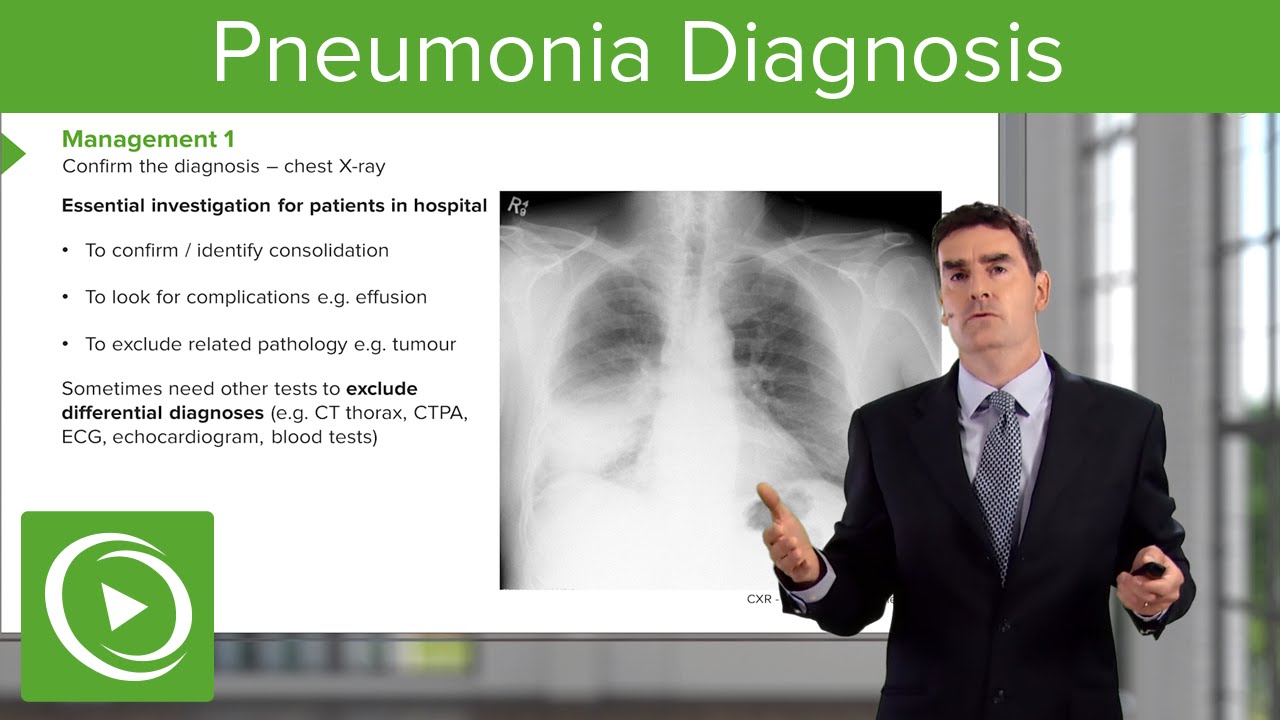
Pneumonia: Diagnosis & Principles of Management – Respiratory Medicine | Lecturio

“Belajar cepat, Menguasai NANDA, NIC, NOC, SDKI, SLKI, dan SIKI dengan Mudah!”
5.0 / 5 (0 votes)
