how a simple programming mistake ended 6 lives
Summary
TLDRThe video recounts the tragic story of Ray Cox, who in 1986 received a fatal overdose of radiation due to a critical software failure in the Therac-25 radiotherapy machine. It explores the technical and human errors behind the incident, including a race condition in the code, inadequate testing, lack of hardware interlocks, and poor safety design. The narrative highlights systemic issues in 1980s software engineering, where assumptions that code couldn’t fail led to catastrophic outcomes. The video underscores the importance of rigorous testing, proper documentation, and robust safety protocols in life-critical systems, drawing lessons still relevant to software engineering today.
Takeaways
- 😀 The East Texas Cancer Treatment Center incident in 1986 led to the death of Ray Cox due to a radiation overdose caused by software bugs in the therak 25 machine.
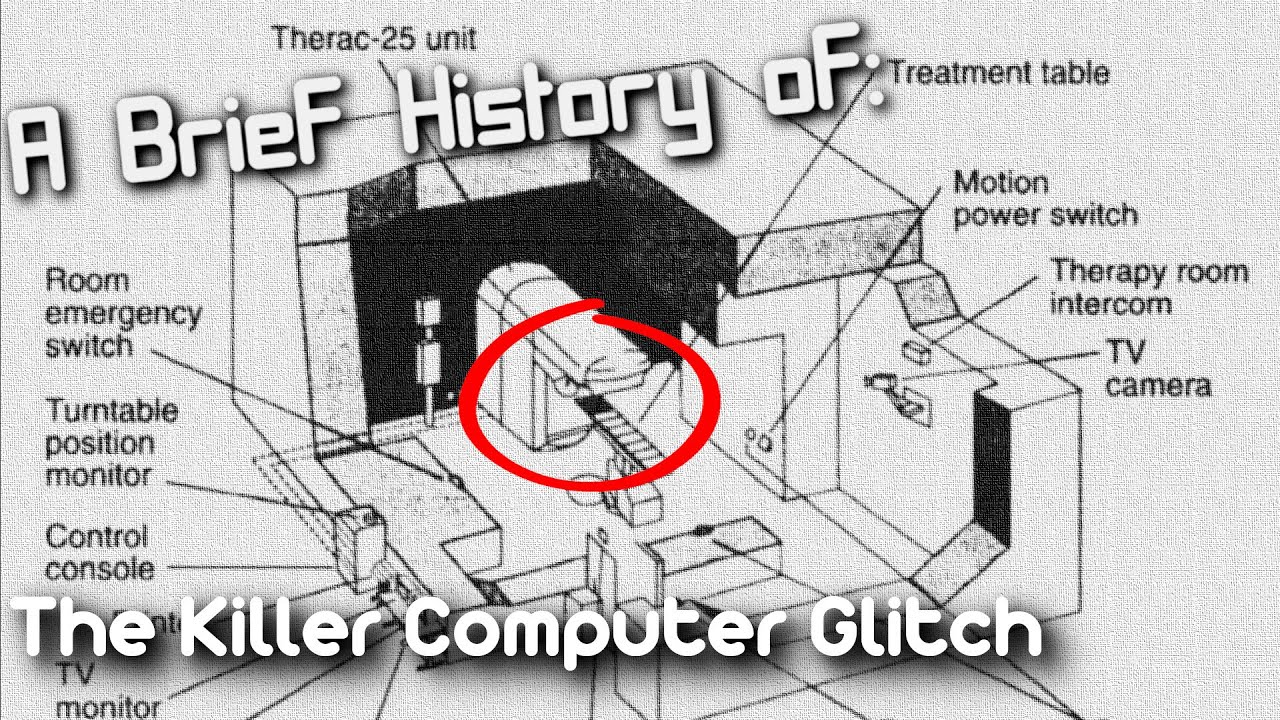
- 😀 The therak 25 machine was developed by Atomic Energy of Canada Limited (AECL) in the 1970s as a more compact and cost-effective radiation therapy solution.
- 😀 The therak 25 was the first radiation therapy machine controlled entirely by software, with no hardware interlocks for safety, making it vulnerable to software errors.
- 😀 Ray Cox's radiation dose was mistakenly set to much higher levels due to a software bug, causing him to receive between 16,000 and 25,000 RADS instead of 180 RADS.
- 😀 The incident led to serious health issues for Ray Cox, including paralysis, pain, and ultimately death five months later from complications.
- 😀 Five other patients in the U.S. and Canada suffered similar fates between 1985 and 1987, all due to the therak 25's software issues.
- 😀 The therak 25 machine lacked proper testing, with only 2,700 hours of testing done by operators and minimal system-level testing after it was assembled in hospitals.
- 😀 One of the key software issues was a race condition, where simultaneous data input and task execution led to incorrect radiation settings being applied.
- 😀 AECL's software engineering practices were poor, with one hobbyist programmer writing the entire code for the therak 25 in assembly language, leading to critical errors.
- 😀 The incident highlighted the need for rigorous software testing, particularly in life-critical systems, and the importance of safety measures beyond just software checks.
Q & A
Who was Ray Cox and what treatment was he scheduled to receive?
-Ray Cox was a patient at the East Texas Cancer Treatment Center who was scheduled to receive 180 RADS of radiation for a tumor developing in his back.
What was the Therak 25, and why was it considered innovative?
-The Therak 25 was a radiation therapy machine developed by AECL that combined X-ray and electron therapy in a single compact machine controlled entirely by software, making it cheaper and easier to use than previous models.
What critical mistake occurred during Ray Cox's treatment?
-The operator initially entered X for X-ray instead of E for electron therapy, and despite quickly correcting it, a race condition in the machine’s software caused Ray Cox to receive a massive overdose of radiation.
What is a race condition, and how did it affect the Therak 25?
-A race condition occurs when two threads in a program access the same data location without proper control, and the outcome depends on which thread executes first. In the Therak 25, it caused misconfiguration of the machine, leading to the delivery of extremely high radiation doses.
How much radiation did Ray Cox actually receive compared to his prescribed dose?
-Ray Cox was prescribed 180 RADS but simulations estimated he actually received between 16,000 and 25,000 RADS, a catastrophic overdose.
What role did hardware interlocks play in previous Therak machines?
-Previous Therak models had hardware interlocks that prevented unsafe radiation levels. These interlocks were removed in the Therak 25 to reduce cost, leaving safety entirely dependent on software.
What safety design issues in Therak 25 contributed to patient deaths?
-The machine lacked hardware safety interlocks, had insufficient system-level documentation, minimal testing, and relied on a single programmer, leading to bugs and unsafe operation under edge conditions.
How did AECL test the Therak 25 before deployment?
-The Therak 25 underwent minimal testing at the hospitals where it was assembled, mostly to confirm basic functionality. There was no extensive regression testing or system-level documentation for error handling.
What were the consequences of the software failure for Ray Cox?
-Ray Cox suffered excruciating pain, paralysis in some areas, and eventually died five months later due to complications from the massive radiation overdose.
How did attitudes toward software reliability in the 1980s contribute to this incident?
-There was a widespread belief that software that worked was infallible, leading to underestimation of risks, insufficient testing, and reliance on a single programmer, which all contributed to unsafe software in the Therak 25.
How many other patients experienced similar incidents with the Therak 25?
-Five other patients in the U.S. and Canada suffered radiation-related injuries or deaths from 1985 to 1987 due to similar software issues in the Therak 25.
What lessons does this incident teach about software safety in medical devices?
-The incident highlights the importance of rigorous testing, hardware fail-safes, documentation, anticipating edge cases, and understanding that software bugs are inevitable, especially in life-critical systems.
Outlines

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowMindmap

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowKeywords

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowHighlights

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowTranscripts

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowBrowse More Related Video

History's Worst Software Error

THERAC-25: O PIOR erro de SOFTWARE da HISTÓRIA
A Brief History of: The killer Therac-25 Radiotherapy machine (Short Documentary)

Medical Mistakes: The Affects on Families

Medical Errors: The Silent Killer in Medicine | Carol Gunn | TEDxFargo
Documentário - O brilho da morte: 30 anos do césio 137
5.0 / 5 (0 votes)