Desequilibrio electrolitico. Hiponatremia, Hipernatremia, Hipokalemia, Hiperkalemia
Summary
TLDRThis video covers the critical role of potassium levels in the body, focusing on the consequences of both hypokalemia (low potassium) and hyperkalemia (high potassium). It explains how these imbalances affect muscle function, the heart's electrical activity, and the importance of monitoring electrocardiograms (ECG) for changes. The script also emphasizes safe potassium replenishment practices, emergency treatment protocols, and various methods for managing potassium levels, such as medication, insulin, bicarbonate, and diuretics. With practical advice for clinical scenarios, the video highlights the importance of individualized care in managing electrolyte disturbances.
Takeaways
- 😀 Hypokalemia (low potassium levels) can cause significant changes in the electrocardiogram (ECG), including ST depression, T wave flattening, and in severe cases, prominent U waves.
- 😀 Potassium levels below 3.0 mEq/L are particularly sensitive and can lead to muscle weakness, ECG alterations, and possible arrhythmias, especially in patients with pre-existing cardiac conditions.
- 😀 It is crucial to monitor potassium levels closely and address any underlying causes, such as vomiting, diarrhea, or certain medications like diuretics or digoxin.
- 😀 Potassium replacement should be done cautiously to avoid complications like phlebitis or arrhythmias. A gradual infusion of potassium is recommended, typically using a solution that is diluted and administered over 4 hours.
- 😀 For urgent potassium replenishment, particularly in diabetic patients with decompensation, intravenous potassium doses can be increased, but must be administered through a central venous catheter to avoid complications.
- 😀 Hyperkalemia (high potassium levels) is defined as a serum potassium level above 5.5 mEq/L and can lead to severe cardiac arrhythmias, such as peaked T waves, QRS widening, and the absence of P waves as potassium levels rise.
- 😀 The primary treatments for hyperkalemia include calcium gluconate (to stabilize the cardiac cell membrane), insulin (to drive potassium into cells), and bicarbonate (to shift potassium into cells).
- 😀 For patients with renal issues or excessive potassium levels, diuretics such as furosemide (loop diuretics) can help eliminate excess potassium from the body, though careful monitoring of dosages is necessary.
- 😀 Intravenous insulin should be used cautiously, starting with lower doses (e.g., 5 units) to prevent sudden hypoglycemia, especially in patients with renal insufficiency.
- 😀 In extreme cases, therapies such as hemodialysis or peritoneal dialysis may be required to directly remove potassium from the body, offering an effective treatment for severe hyperkalemia.
- 😀 Resins like Kayexalate can also be used to bind potassium in the gastrointestinal tract, though availability in hospitals may vary, and they are not always the first-line treatment.
Q & A
What is the primary focus of the transcript?
-The transcript focuses on the clinical significance of potassium imbalances, specifically hypokalemia and hyperkalemia, and their effects on the electrocardiogram (ECG). It also discusses how to manage and treat these conditions, particularly in patients with cardiac issues or renal disease.
How does hypokalemia manifest on an ECG?
-Hypokalemia, or low potassium levels, manifests on an ECG with changes such as depression of the ST segment, a low amplitude of the T wave, and in severe cases, flattening of the T wave. As potassium levels drop, these changes become more pronounced, especially when potassium levels fall below 3.0 mEq/L.
What are common symptoms associated with low potassium?
-Common symptoms of hypokalemia include muscle weakness, ascending muscle paralysis, fatigue, nausea, vomiting, and in severe cases, cardiac arrhythmias.
Why is potassium replacement important in hypokalemia?
-Potassium replacement is critical because low potassium levels can lead to serious complications such as muscle weakness, arrhythmias, and even cardiac arrest. Restoring potassium to normal levels helps prevent these adverse effects and stabilizes the patient's condition.
What precautions should be taken when administering potassium replacement?
-When administering potassium replacement, care must be taken to avoid complications such as phlebitis or pain at the infusion site. Potassium should be given slowly and in proper dilution to minimize the risk of cardiac arrhythmias. The infusion should be monitored, especially in patients with heart conditions.
How should potassium be administered to a patient with hypokalemia?
-Potassium should be administered intravenously in a solution with appropriate dilution, typically at a rate of 10-20 mEq per hour. In urgent cases, higher doses can be given but must be done through a central venous catheter to avoid complications like peripheral vein irritation.
What is the role of calcium gluconate in treating hyperkalemia?
-Calcium gluconate acts as a membrane stabilizer, reducing the risk of arrhythmias in patients with elevated potassium levels. It does not lower potassium levels but helps stabilize the cell membranes to prevent cardiac disturbances. It is typically given intravenously in doses of 10-30 mL of a 10% solution.
How does salbutamol help in managing hyperkalemia?
-Salbutamol, a beta-agonist, helps lower potassium levels by shifting potassium from the bloodstream into cells. It can be administered intravenously (0.5 mg in 100 mL glucose) or by inhalation (10-20 mg), and its effects typically start within 30 minutes, lasting for 2-3 hours.
What is the role of insulin in treating hyperkalemia?
-Insulin helps lower serum potassium by promoting the cellular uptake of potassium. In the case of hyperkalemia, insulin is administered with glucose to prevent hypoglycemia. Typically, 5-10 units of rapid-acting insulin are used with 50% dextrose, and its effects begin in about 15 minutes, lasting for 6-8 hours.
What are the consequences of not properly managing potassium imbalances?
-Failure to manage potassium imbalances, especially severe hypokalemia or hyperkalemia, can result in serious complications such as muscle paralysis, arrhythmias, cardiac arrest, and even death. Proper diagnosis and timely treatment are crucial to prevent these life-threatening conditions.
Outlines

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowMindmap

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowKeywords

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowHighlights

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowTranscripts

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowBrowse More Related Video

Fluid & Electrolytes Nursing Students Hyperkalemia Made Easy NCLEX Review

Hypokalemia Symptoms and Treatment | Nursing School Lecture

Dealing With Diuretics | NurseInTheMaking | NCLEX Pharmacology | Registered Nurse
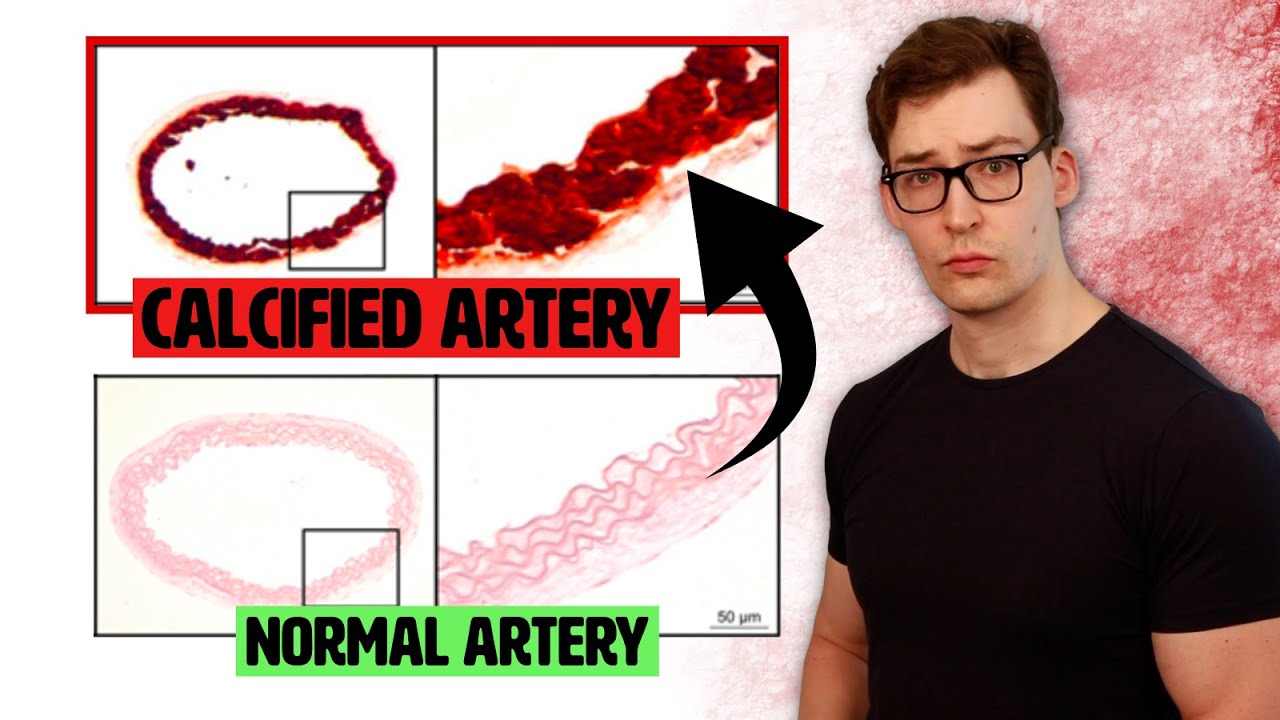
This Mineral Deficiency is causing Calcified Arteries.
Can the "opposite" of salt fix blood pressure?
ELECTROLYTE IMBALANCES (MADE EASY) #Electrolyteimbalances #Electrolytes #Electrolyteimbalance
5.0 / 5 (0 votes)