Septic Shock
Summary
TLDRThis ICU curriculum session focuses on defining sepsis and septic shock, outlining their clinical manifestations, and detailing treatment protocols. It emphasizes the importance of early recognition and management, including prompt administration of broad-spectrum antibiotics, fluid resuscitation with lactated ringers, and vasopressors like norepinephrine and vasopressin. The session also discusses the role of corticosteroids in refractory septic shock and the significance of source control. A case study illustrates the application of these principles in managing a patient with suspected pyelonephritis.
Takeaways
- 📚 The session focuses on defining sepsis and septic shock according to the Sepsis-3 definitions.
- 🩺 Septic shock is a subset of sepsis characterized by underlying circulatory and cellular metabolic abnormalities that significantly increase mortality.
- 🌡 Clinically, septic shock is identified by sepsis plus hypotension that does not improve despite fluid resuscitation, and a serum lactate level >2 mmol/L.
- 🚨 Sepsis is a time-sensitive medical emergency requiring prompt recognition and management to improve patient outcomes.
- 💊 Early administration of broad-spectrum antibiotics is crucial in the treatment of septic shock, with each hour's delay increasing the risk of in-hospital mortality.
- 💧 The initial fluid resuscitation for sepsis or septic shock involves a 30 mL/kg bolus of intravenous fluid, typically lactated Ringer's solution.
- 💊 Vasopressors are used to maintain a mean arterial pressure (MAP) ≥65 mmHg, with norepinephrine being the first-line agent.
- 🔍 Source control, including broad cultures and imaging, is essential in managing septic shock to identify and treat the infection site.
- 🩹 Corticosteroids, such as hydrocortisone, are considered for patients with vasopressor-refractory septic shock to improve vasopressor responsiveness.
- 📈 The session emphasizes the importance of continuous assessment and monitoring of patients in septic shock, including mental status, perfusion, urine output, and lab trends.
Q & A
What are the objectives of the fifth session in the ICU curriculum?
-The objectives are to define sepsis and septic shock according to Sepsis-3 definitions, describe the pathophysiologic abnormalities and clinical manifestations of septic shock, and to describe the treatment principles for a patient in septic shock including appropriate antibiotics, fluid resuscitation, and vasopressors.
How is sepsis defined according to the Sepsis-3 task force definition from 2016?
-Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection.
What are the clinical criteria used to identify sepsis before the Sepsis-3 definition?
-Before the Sepsis-3 definition, sepsis was identified using the SIRS criteria, which include temperature greater than 38 or less than 36 degrees Celsius, heart rate greater than 90 beats per minute, respiratory rate greater than 20 breaths per minute, and white blood cell count greater than 12,000 or less than 4,000 or greater than 10 percent bands.
What is the qSOFA score and how is it used?
-qSOFA stands for quick Sequential Organ Failure Assessment and is used to identify patients with suspected infection likely to have sepsis or patients with sepsis at high risk of deterioration or poor outcome. It is composed of three variables: systolic hypotension less than 100 mmHg, respiratory rate greater than 22 breaths per minute, and altered mental status.
What is the clinical definition of septic shock according to the Sepsis-3 guidelines?
-Septic shock is defined as sepsis with persistent hypotension requiring vasopressors to maintain a mean arterial pressure (MAP) of at least 65 mmHg and a serum lactate greater than 2 mmol/L despite adequate fluid resuscitation.
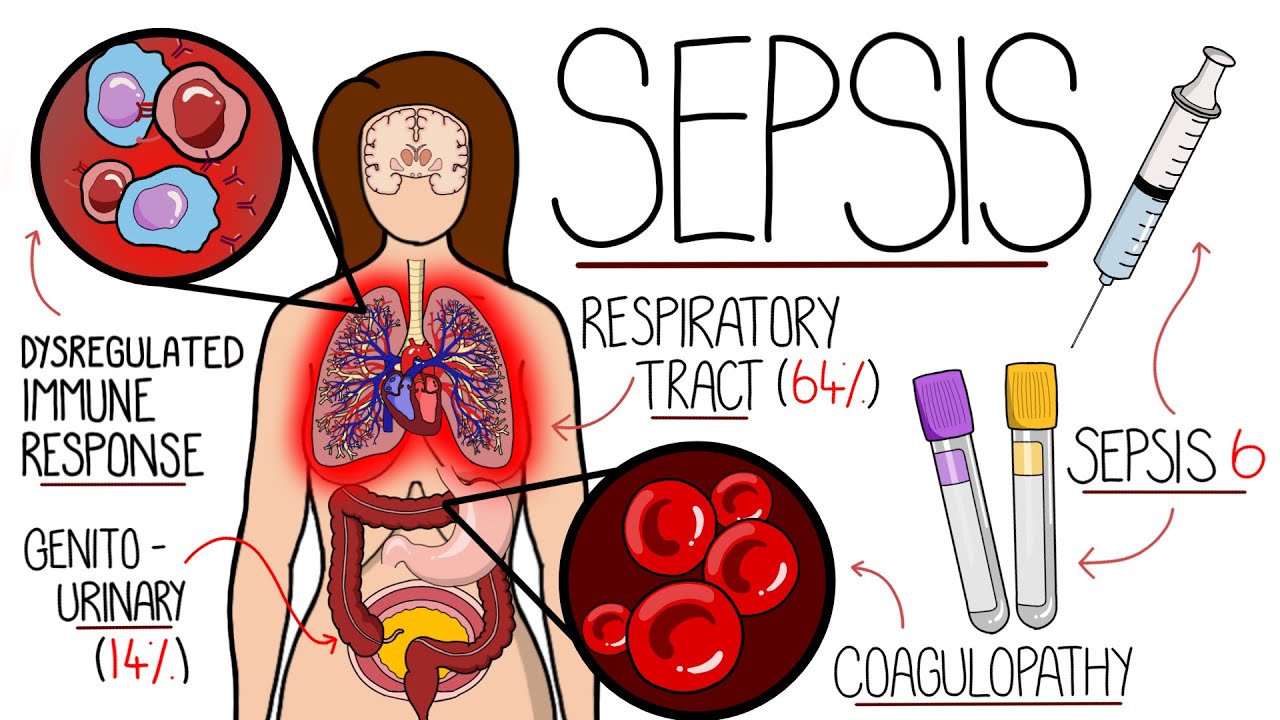
What types of infections are most commonly associated with sepsis?
-Sepsis is most commonly caused by infections of the respiratory system, followed by infections of the gastrointestinal and genitourinary systems.
What are the clinical manifestations of septic shock?
-Clinical manifestations of septic shock include hypotension, tachycardia, altered mental status, and signs of poor perfusion such as mottling or oliguria.
What are the four main principles in the management of septic shock?
-The four main principles in the management of septic shock are early antibiotics, fluid resuscitation, vasopressors, and source control.
What is the recommended initial fluid resuscitation for patients with sepsis or septic shock?
-Patients with sepsis or septic shock should receive a bolus of 30 mL/kg of intravenous fluid for initial volume resuscitation.
Which vasopressor is typically used first in the treatment of septic shock, and why?
-Norepinephrine is typically used first in the treatment of septic shock because it is a predominant alpha-1 agonist with some additional beta agonist effects, and it has been shown to be effective in maintaining blood pressure without increasing the risk of arrhythmias compared to other vasopressors like dopamine.
What is the role of corticosteroids in the treatment of septic shock?
-Corticosteroids are typically reserved for patients in vasopressor-refractory septic shock. They may improve vasopressor responsiveness and have been associated with faster resolution of shock, more ventilator-free days, and decreased ICU length of stay.
Outlines

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowMindmap

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowKeywords

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowHighlights

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowTranscripts

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowBrowse More Related Video

Understanding Sepsis & Septic Shock (Visual Guide) | 2024 Updated Tutorial

Septic Shock | Shock (Part 8)

SHOCK: Types, Pathogenesis of Septic Shock

Choque Séptico - Fisiopatologia, sinais e sintomas e tratamento! #enfermagem #enfermeiro
Understanding Sepsis (Sepsis Explained Clearly)

Cara Cepat Infus/Terapi Cairan di IGD | Fluid Therapy in Emergency Settings Made Incredibly Easy
5.0 / 5 (0 votes)