An Approach to Vertigo
Summary
TLDRThis video by Eric from Strong Medicine offers a comprehensive guide on diagnosing vertigo, distinguishing it from lightheadedness and disequilibrium, which are often confused with dizziness. It outlines the differences, common causes of vertigo such as BPPV and Meniere's disease, and emphasizes the importance of the Hints exam in identifying central versus peripheral causes. The video also provides an evaluation algorithm and highlights the necessity of considering neuroimaging to rule out serious conditions like stroke.
Takeaways
- 📝 Dizziness is a nonspecific term that can refer to vertigo, pre-syncope, or disequilibrium, and it's crucial to distinguish between these conditions for accurate diagnosis.
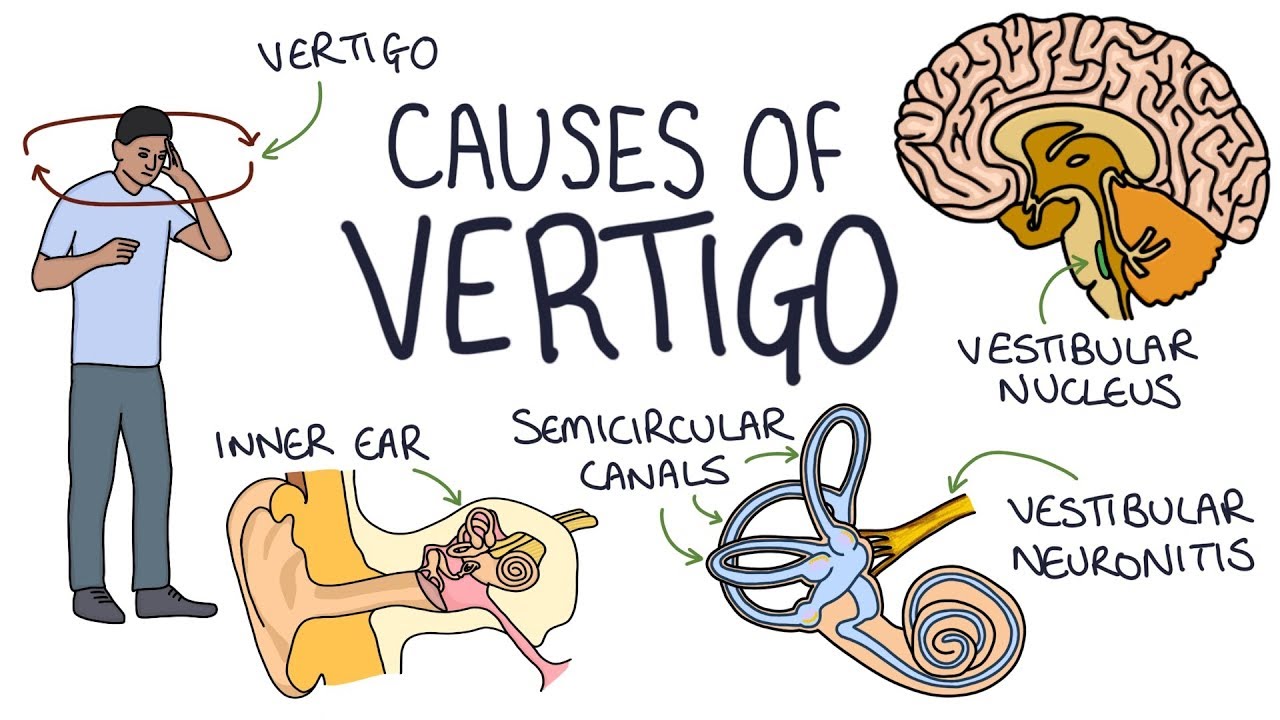
- 🎢 Vertigo is characterized by the illusion of motion while stationary, often described as a spinning sensation, and is associated with nausea due to disruptions in vestibular pathways.
- 🕊 Benign Paroxysmal Positional Vertigo (BPPV) is the most common cause of vertigo, caused by dislodged otolith crystals in the semicircular canals, and is diagnosed using the Dix-Hallpike maneuver.
- 🌀 Meniere's disease is another cause of episodic vertigo, associated with progressive hearing loss and tinnitus, and is suggested by symptoms like episodic hearing loss and tinnitus.
- 💉 Vestibular neuritis, likely due to viral inflammation, is a common peripheral cause of vertigo that can be distinguished from central causes through physical examination.
- 🏥 Central causes of vertigo, such as stroke or multiple sclerosis, are less common but require immediate attention, and may necessitate brain MRI or MRA for diagnosis.
- 🔍 The history and physical examination are primarily used to diagnose vertigo, with blood tests being rarely helpful, and imaging reserved for suspected central causes.
- 👁️ The head impulse test, nystagmus examination, and test of skew, collectively known as the HINTS exam, are critical for differentiating between central and peripheral vertigo.
- 🚑 An abnormal HINTS exam, especially in older patients with stroke risk factors or additional neurologic symptoms, should prompt immediate neuroimaging to rule out central causes like stroke.
- 📉 Audiometry is important when Meniere's disease is suspected, helping to distinguish it from other causes of vertigo based on hearing test results.
- 🔄 The diagnostic approach to vertigo involves a stepwise evaluation starting from patient history, physical examination, and specific maneuvers, followed by additional tests as needed based on the suspected cause.
Q & A
What is the main difference between vertigo, lightheadedness, and disequilibrium?
-Vertigo is the illusion of motion while stationary, often described as a spinning sensation. Lightheadedness, or pre-syncope, is the sensation of transiently slowed consciousness or feeling faint, which can progress to a brief loss of consciousness. Disequilibrium is difficulty maintaining balance, usually associated with frequent falls without loss of consciousness.
What is the most common symptom associated with vertigo?
-The most frequently associated symptom with vertigo is nausea.
How can benign paroxysmal positional vertigo (BPPV) be triggered?
-BPPV can be triggered by changes in head position, such as moving from lying to sitting or standing, or when turning the head while supine.
What is Meniere's disease and what are its typical symptoms?
-Meniere's disease is believed to be associated with an increased volume of endolymph, a fluid in the inner ear. Symptoms include discrete episodes of vertigo lasting between 20 minutes and a day, progressive hearing loss, and tinnitus.
What is the general mechanism behind lightheadedness?
-The general mechanism of lightheadedness is a transient reduction of cerebral perfusion.
What is vestibular neuritis and what is its likely cause?
-Vestibular neuritis is a benign self-limited disorder thought to be most likely due to viral or post-viral inflammation of one or both vestibular nerves.
How can an acoustic neuroma present symptoms of vertigo?
-An acoustic neuroma, also known as a vestibular schwannoma, is a benign tumor of the vestibular nerve. As it grows slowly, unilateral hearing loss is a more common symptom than vertigo, but the central vestibular centers can adapt to the lack of unilateral vestibular inputs.
What is the purpose of the Dix-Hallpike maneuver in the evaluation of vertigo?
-The Dix-Hallpike maneuver is a test specifically for BPPV. It helps to confirm the diagnosis of BPPV by inducing nystagmus with the maneuver.
What does the HINTS exam stand for and why is it important in the evaluation of vertigo?
-The HINTS exam stands for Head Impulse, Nystagmus, and Test of Skew. It is important in the evaluation of vertigo because it helps to distinguish central from peripheral causes of vertigo with high predictive values.
What are some additional tests that might be indicated in the evaluation of vertigo?
-Additional tests that might be indicated include audiometry for suspected Meniere's disease, and a brain MRI plus or minus MRA if a central cause cannot be ruled out from the history and exam alone.
What is the key takeaway from the video regarding the evaluation of vertigo?
-The key takeaway is that the diagnosis of vertigo is predominantly based on history and physical exam, with the HINTS exam being an important component. An abnormal HINTS exam should warrant an MRI plus or minus an MRA to look for central causes such as a posterior circulation stroke or multiple sclerosis.
Outlines

このセクションは有料ユーザー限定です。 アクセスするには、アップグレードをお願いします。
今すぐアップグレードMindmap

このセクションは有料ユーザー限定です。 アクセスするには、アップグレードをお願いします。
今すぐアップグレードKeywords

このセクションは有料ユーザー限定です。 アクセスするには、アップグレードをお願いします。
今すぐアップグレードHighlights

このセクションは有料ユーザー限定です。 アクセスするには、アップグレードをお願いします。
今すぐアップグレードTranscripts

このセクションは有料ユーザー限定です。 アクセスするには、アップグレードをお願いします。
今すぐアップグレード関連動画をさらに表示

Stop Vertigo or Dizziness in 90 Seconds With 3 Acupressure Points

What is Vertigo and What Causes it? | Benign Paroxysmal Positional Vertigo | The Dr. Binocs Show

The Head Impulse Test

Vertigo: Causes, Pathophysiology and Treatments, Animation

How to Get Rid of Cervicogenic Dizziness | Cervical Dizziness Exercises | Dr. Jon Saunders
Understanding the Causes of Vertigo
5.0 / 5 (0 votes)
