Shoulder joint: Movements, bones and muscles - Human Anatomy | Kenhub
Summary
TLDRThis tutorial offers a detailed exploration of the shoulder (glenohumeral) joint from a lateral perspective, highlighting its bones, joint cavity, ligaments, muscles, and bursae. It explains how the humerus and scapula interact, the role of the glenoid labrum, and the joint capsule in stability. Key ligaments, including the coracohumeral and glenohumeral ligaments, and muscles such as the rotator cuff, teres major, and long heads of biceps and triceps, are examined. The video also covers bursae like the subacromial and subscapularis bursae, and clinical correlations, including subacromial bursitis and painful arc syndrome, equipping learners to understand both anatomy and common injuries.
Takeaways
- 💪 The shoulder joint, also called the glenohumeral joint, is a ball-and-socket synovial joint, providing a wide range of movements including flexion, extension, abduction, adduction, rotation, and circumduction.
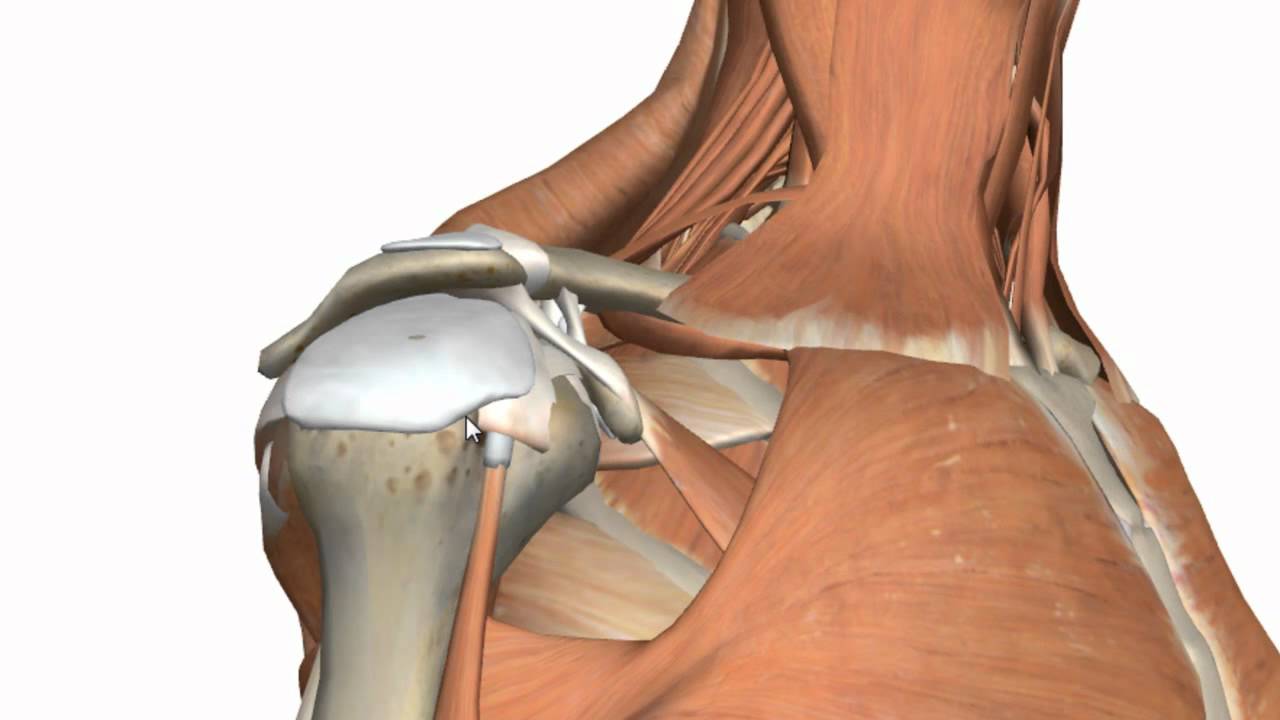
- 🦴 The joint is formed by the humerus and the scapula, with key features including the humeral head, greater and lesser tubercles, intertubercular groove, anatomical neck, and the scapula’s glenoid cavity, acromion, and coracoid processes.
- 🔍 The glenoid cavity is shallow and smaller than the humeral head, which provides mobility but reduces inherent stability, requiring support from surrounding muscles and ligaments.
- 🛡️ The glenoid labrum, a fibrocartilaginous ring around the glenoid cavity, helps deepen the socket and increase joint stability.
- 🦵 The joint capsule surrounds the humeral head, consisting of an outer fibrous layer and an inner synovial membrane that secretes fluid for lubrication.
- 🔗 Key ligaments stabilizing the shoulder include the coracohumeral ligament, superior, middle, and inferior glenohumeral ligaments, and the coracoacromial ligament which forms a superior arch over the joint.
- 🏋️ The rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) create compressive forces around the humeral head, ensuring stability and centering it in the glenoid cavity.
- 💥 Additional muscles contributing to shoulder stability include the teres major, long head of the triceps brachii, and long head of the biceps brachii, each with specific origins and insertions influencing movement and stabilization.
- 🩹 Bursae, such as the subacromial bursa and subtendinous bursa of the subscapularis, act as cushions to reduce friction between tendons, muscles, and bones, aiding smooth movement of the joint.
- ⚠️ Clinical relevance: Subacromial bursitis can cause painful arc syndrome, characterized by pain during shoulder abduction between 60 and 120 degrees, often due to overuse or trauma.
Q & A
What type of joint is the shoulder (glenohumeral) joint and what movements does it allow?
-The shoulder joint is a ball-and-socket synovial joint. It allows a wide range of movements including flexion, extension, abduction, adduction, medial and lateral rotation, and circumduction.
Which two bones form the shoulder joint and what are their key features relevant to the joint?
-The shoulder joint is formed by the humerus and the scapula. Key features include the humeral head, greater and lesser tubercles, intertubercular groove, and anatomical neck of the humerus; and the glenoid cavity, supraglenoid and infraglenoid tubercles, acromion process, and coracoid process of the scapula.
Why does the shoulder joint rely more on muscles and ligaments than on bony structures for stability?
-The glenoid cavity is shallow and has a surface area about one-fourth that of the humeral head. This results in a small contact area, which allows high mobility but compromises bony stability, making muscles and ligaments essential for joint support.
What is the function of the glenoid labrum in the shoulder joint?
-The glenoid labrum is a fibrocartilaginous ring around the glenoid fossa that deepens the socket, improving the functional stability of the shoulder joint by increasing the contact area with the humeral head.
Name the main ligaments supporting the shoulder joint and their primary functions.
-Key ligaments include the coracohumeral ligament (prevents inferior displacement of the humerus), the superior, middle, and inferior glenohumeral ligaments (strengthen anterior and inferior aspects of the joint), and the coracoacromial ligament (forms a protective arch over the humeral head).
Which muscles comprise the rotator cuff, and how do they contribute to shoulder stability?
-The rotator cuff muscles are the supraspinatus, infraspinatus, teres minor, and subscapularis. They create a compressive force around the humeral head, centering it within the glenoid cavity and stabilizing the shoulder in all positions.
What is the role of the teres major, long head of triceps brachii, and long head of biceps brachii in shoulder stability?
-These muscles assist in shoulder stability by providing additional muscular support. Teres major stabilizes inferiorly, the long head of the triceps originates from the infraglenoid tubercle, and the long head of the biceps originates from the supraglenoid tubercle, helping to maintain humeral alignment.
Describe the function and location of the subacromial and subdeltoid bursae.
-The subacromial bursa lies between the acromion, coracoacromial ligament, and the supraspinatus tendon, reducing friction during abduction. The subdeltoid bursa is continuous with the subacromial bursa and lies beneath the deltoid muscle to prevent friction with underlying structures.
What is subacromial bursitis and how does it cause 'painful arc syndrome'?
-Subacromial bursitis is inflammation of the subacromial bursa, often due to overuse or trauma. Painful arc syndrome occurs when the arm is abducted between 60° and 120°, as the inflamed bursa and supraspinatus tendon are compressed, causing pain. Pain is minimal outside this range.
How does the subtendinous bursa of the subscapularis differ from the subacromial bursa in terms of joint communication?
-The subtendinous bursa of the subscapularis communicates with the glenohumeral joint, meaning infection can spread into the joint. In contrast, the subacromial bursa normally does not communicate with the joint capsule, so infection is less likely to spread.
From a lateral view, how can you distinguish the anterior and posterior aspects of the shoulder joint?
-In a lateral view, the anterior aspect of the shoulder joint is on the right side of the image, while the posterior aspect is on the left side. Key landmarks such as the coracoid process (anterior) and acromion process (posterior) help identify these aspects.
Outlines

Dieser Bereich ist nur für Premium-Benutzer verfügbar. Bitte führen Sie ein Upgrade durch, um auf diesen Abschnitt zuzugreifen.
Upgrade durchführenMindmap

Dieser Bereich ist nur für Premium-Benutzer verfügbar. Bitte führen Sie ein Upgrade durch, um auf diesen Abschnitt zuzugreifen.
Upgrade durchführenKeywords

Dieser Bereich ist nur für Premium-Benutzer verfügbar. Bitte führen Sie ein Upgrade durch, um auf diesen Abschnitt zuzugreifen.
Upgrade durchführenHighlights

Dieser Bereich ist nur für Premium-Benutzer verfügbar. Bitte führen Sie ein Upgrade durch, um auf diesen Abschnitt zuzugreifen.
Upgrade durchführenTranscripts

Dieser Bereich ist nur für Premium-Benutzer verfügbar. Bitte führen Sie ein Upgrade durch, um auf diesen Abschnitt zuzugreifen.
Upgrade durchführenWeitere ähnliche Videos ansehen
Shoulder Joint - Glenohumeral Joint - 3D Anatomy Tutorial

Anatomy of the Shoulder Joint | Bones, Ligaments, and Muscles

Elbow Joint: Bones, Muscles & Movement - Human Anatomy | Kenhub
Hip Anatomy Animated Tutorial
Anatomy of the Hip Joint | Bones, Ligaments, & Muscles

SHOULDER JOINT INTRODUCTION (SHOULDER JOINT COMPLEX BIOMECHANICS)Physiotherapy Tutorials
5.0 / 5 (0 votes)
