SOAP NOTES
Summary
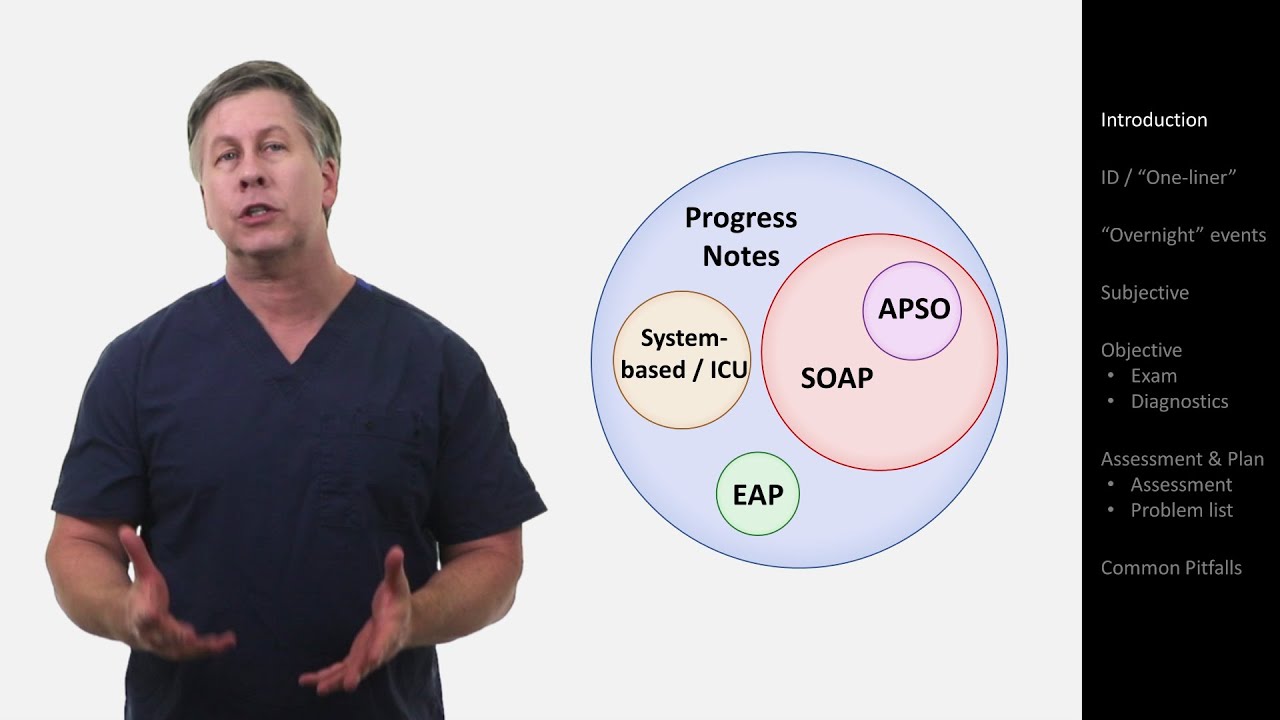
TLDRThis video script offers a fundamental introduction to SOAP notes, a critical documentation tool in healthcare settings. It outlines the structure and purpose of SOAP notes, emphasizing their role in patient record-keeping and interprofessional communication. The acronym SOAP stands for Subjective, Objective, Assessment, and Plan, with each section containing specific subparts tailored to the patient's needs. The script walks through an example SOAP note for a 62-year-old male with a sore throat, detailing each section's content, from the patient's reported symptoms to the healthcare provider's assessment and proposed treatment plan.
Takeaways
- 📝 SOAP notes are essential for documentation and communication in healthcare settings, serving as a permanent medical record of patient interactions.
- 🔤 The acronym SOAP stands for Subjective, Objective, Assessment, and Plan, which are the four main parts of a SOAP note.
- 🗣️ The Subjective section includes patient-reported information such as symptoms, their severity, and timing, gathered through conversation and medical record review.
- 🔍 The Objective section records the healthcare provider's observations and findings from the physical examination, excluding patient-reported information.
- 🏥 The Assessment part synthesizes information from the Subjective and Objective sections to form a professional judgment about the patient's condition.
- 📋 The Plan outlines the actions to be taken, which may include treatment plans, prescriptions, referrals, patient education, and follow-up instructions.
- 👨⚕️ SOAP notes are used across various healthcare disciplines and can vary in length and detail depending on the situation.
- 📚 A comprehensive SOAP note, often referred to as a history and physical, reviews and documents all possible sections, while more focused notes may only include relevant sections.
- 👴 The example provided illustrates a SOAP note for a 62-year-old male with a sore throat, including his chief complaint, history of present illness, examination findings, and the subsequent plan of action.
- 💊 The plan may involve specific treatments like prescriptions, lifestyle advice, and follow-up appointments, tailored to the patient's diagnosed condition.
Q & A
What is the primary purpose of SOAP notes in healthcare settings?
-SOAP notes are used for documentation and communication, providing a record of patient interactions that becomes part of their permanent medical records, and facilitating communication with future caregivers.
What does SOAP stand for in healthcare documentation?
-SOAP stands for Subjective, Objective, Assessment, and Plan, which are the four main parts of a SOAP note.
What kind of information should be included in the Subjective section of a SOAP note?
-The Subjective section should contain information gathered from talking to the patient, family members, and medical record review, including the patient's symptoms, their timing, severity, and any associated or absent symptoms.
How should the Objective section of a SOAP note differ from the Subjective section?
-The Objective section should only contain the healthcare provider's physical findings and observations, such as vital signs, general appearance, and results from systems examinations, without any patient-reported information.
What is the purpose of the Assessment section in a SOAP note?
-The Assessment section combines information from the Subjective and Objective sections to determine what the healthcare provider thinks is going on with the patient, which may include a differential diagnosis and billable medical diagnoses.
What actions can be included in the Plan section of a SOAP note?
-The Plan section outlines the actions to be taken, which may include ordering prescriptions, requesting consultations, providing patient education, setting follow-up appointments, and managing the patient's condition with treatments and diagnostics.
Why is it important to be concise when documenting the Chief Complaint in the SOAP note?
-Being concise helps ensure that only the most important information is summarized, making it easier for future healthcare providers to quickly understand the patient's primary concern.
Can you provide an example of how to document a patient's history of present illness in the SOAP note?
-An example includes noting the patient's age, existing medical conditions, the chief complaint, the severity and duration of symptoms, associated symptoms, and any relevant medical history or allergies.
What should be included in the General Survey when documenting a patient's examination in the Objective section?
-The General Survey should comment on the patient's overall appearance, level of consciousness, and any signs of distress.
How does the healthcare provider use the information from the Objective section to form an Assessment in the SOAP note?
-The healthcare provider uses the objective findings to support or refute the subjective information, leading to a clinical picture that helps in formulating a diagnosis and differential diagnoses.
Why is it important to include follow-up instructions in the Plan section of a SOAP note?
-Follow-up instructions are important to ensure the patient's condition is monitored and managed effectively, and to provide guidance on when to seek further medical attention if the condition changes or does not improve.
Outlines
This section is available to paid users only. Please upgrade to access this part.
Upgrade NowMindmap

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowKeywords

This section is available to paid users only. Please upgrade to access this part.
Upgrade NowHighlights
This section is available to paid users only. Please upgrade to access this part.
Upgrade NowTranscripts
This section is available to paid users only. Please upgrade to access this part.
Upgrade NowBrowse More Related Video





5.0 / 5 (0 votes)